It feels like every case in the office now has a surgical intervention for a Shoulder tear or Knee tear. With the advent of "Surgicenters", Day-op arthroscopic procedures have become the norm, changing the landscape of personal injury cases. What was purely a soft-tissue case with conservative treatment, can now be touted to the jury as a "SURGERY", requiring a six-figure recovery. Knowing your anatomy in this type of case is critical to the defense. Consider the transcript attached from the direct and cross-examination of Dr. Sanford Wert in a Queens case from August 2015 where Tim Jones from our office received a great result. The jury awarded $75,000 to the plaintiff who claimed a shoulder tear with surgery. The plaintiff turned down $100,000 and asked the Jury for a $600,000 verdict.
Rotator cuff impingement syndrome and associated rotator cuff tears are common conditions, treated across the country every day, outside of litigation. Typical Symptoms include pain, weakness and loss of motion. Causes of impingement syndrome include calcified coracoacromial ligament, acromioclavicular joint arthritis, structural abnormalities of the acromion and weakness of the rotator cuff muscles.
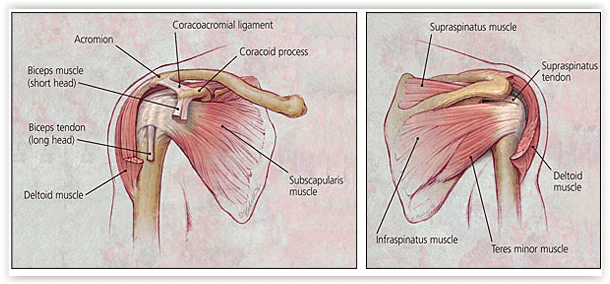
Anatomy
The rotator cuff comprises four muscles - the subscapularis, the supraspinatus, the infraspinatus and the teres minor-and their musculotendinous attachments. The subscapularis muscle is innervated by the subscapular nerve and originates on the scapula. It inserts on the lesser tuberosity of the humerus. The supraspinatus and infraspinatus are both innervated by the suprascapular nerve, originate in the scapula and insert on the greater tuberosity. The teres minor is innervated by the axillary nerve, originates on the scapula and inserts on the greater tuberosity. The subacromial space lies underneath the acromion, the coracoid process, the acromioclavicular joint, and the coracoacromial ligament. A bursa in the subacromial space provides lubrication for the rotator cuff. Understanding the functional anatomy of the rotator cuff is critical. The rotator cuff is what stabilizes the ball and socket shoulder joint. The fixed stabilizers are the capsule and the labrum complex, including the glenohumeral ligaments.
On cross-examination of the plaintiff's expert orthopedist, you can explore all of the "non-traumatic" causes of a rotator cuff tear including:
Thick subacromial bursa
Acromial defects (os acromiale)
Anterior or posterior capsular contractures (adhesive capsulitis)
Secondary impingement from unstable shoulder
Degenerative Loss of rotator cuff causing superior migration of humerus (tear, loss of strength)
Nonoutlet impingement
Thickened or calcified coracoacromial ligament
Osteoarthritic spurs of acromioclavicular joint (includes subacromial spurs)
Type 2 and type 3 acromions
Subacromial spurs
Outlet impingement
You need to explore a differential diagnosis which would include all the non-traumatic findings listed above. If you do your homework, you can plant significant doubt in the plaintiff's theory of the case that the injury was caused by trauma.